Heart Health
Understanding Your Cholesterol Report
Written by - Dr. Nimisha Gupta, M.D. Pathology
12 min read
A cholesterol report may look complex, but once you understand what each number means, it becomes a valuable tool for understanding and managing your heart health.

Before you start: This guide is for general education. It explains how to understand your Cholesterol Report, but it is not a substitute for advice from your own doctor, who knows your full history. Treatment targets and next steps should always be set with a qualified clinician. Cholesterol is a sensitive issue for many people. If reading yours brings up worry, that is a good reason to talk it through with your care team rather than sit with it alone.
Most of us have held a lipid profile report in our hands at some point, scanned the row of numbers, noticed a value or two flagged in red, and then waited for the doctor to tell us whether to worry. But a cholesterol report is not as intimidating as it looks. Once you understand what each line is measuring and why it matters, you can read your own report intelligently, ask better questions, and take charge of your heart health. This matters especially for people of Indian and South Asian origin. We tend to develop heart disease roughly a decade earlier than Western populations, often at lower cholesterol levels and lower body weights, and frequently without the classic warning signs. Because of this, the Lipid Association of India (LAI) recommends more aggressive cholesterol targets than most Western guidelines. Understanding your numbers is the first step toward protecting yourself. This guide walks you through the basic lipid profile, the newer extended (advanced) lipid profile, important markers your standard report may not include — apolipoprotein B, lipoprotein(a), apolipoprotein A1, and the powerful ApoB/ApoA1 ratio — the physical signs that lipids can leave on the body, and a set of common questions and answers.
First,What Is Cholesterol?
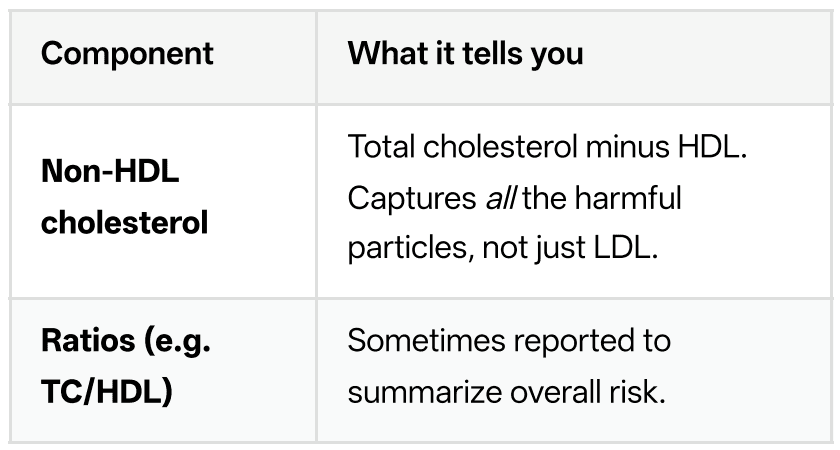
Cholesterol is a waxy, fat-like substance your body needs to build cells, make hormones, and produce vitamin D. Your liver makes most of it; the rest comes from food. Because cholesterol doesn't dissolve in blood, it travels packaged inside particles called lipoproteins. The main ones your report cares about are:
LDL (low-density lipoprotein) — often called "bad" cholesterol. LDL particles deposit cholesterol into artery walls, where it builds up as plaque. This is the primary driver of heart attacks and strokes.
HDL (high-density lipoprotein) — often called "good" cholesterol. HDL helps carry cholesterol away from the arteries back to the liver.
VLDL (very-low-density lipoprotein) — carries triglycerides and is also atherogenic (plaqueforming).
Triglycerides — a type of fat used for energy.
High levels, common with a sugar- and carbohydrate-heavy diet, add to cardiovascular risk. The goal of a lipid profile is to measure the balance between the particles that harm your arteries and those that protect them.
The Basic Lipid Profile
This is the standard, widely available, and inexpensive test that most people get. A basic lipid profile typically reports five to six values:

A note on fasting: For years we were told to fast 9–12 hours before a lipid test. The LAI now considers a non-fasting sample good enough for managing most patients, which makes testing far more convenient. Fasting is still preferred when triglycerides are very high or when the doctor specifically requests it. As a rule of thumb, triglycerides of 150 mg/dL or more when fasting, or 175 mg/dL or more when non-fasting, are treated as a warning sign that adds to cardiovascular risk.
The basic profile is excellent for screening the general population and for tracking whether treatment is working. But it has blind spots — and that is where the extended profile comes in.
The Extended (Advanced) Lipid Profile
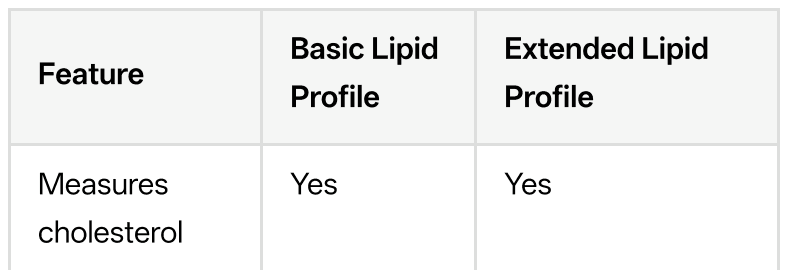
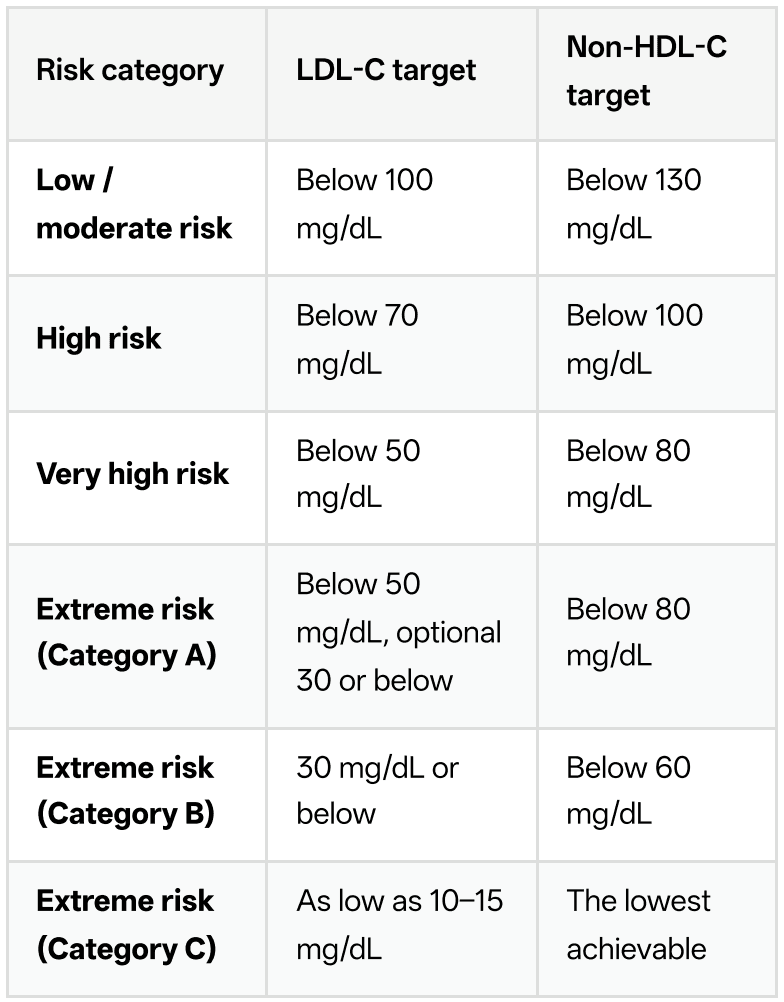
An extended lipid profile includes everything in the basic panel and adds markers that reveal risk the standard test can miss. Two people can have identical LDL numbers but very different real risk, and the extended panel helps explain why. Depending on the laboratory, an extended profile may add:
Apolipoprotein B (ApoB) — the actual number of harmful particles.
Apolipoprotein A1 (ApoA1) — the main protein of protective HDL particles.
The ApoB/ApoA1 ratio — the balance of "bad" to "good" particles in a single number.
Lipoprotein(a), or Lp(a) — an inherited, independent risk factor.
Direct LDL, VLDL cholesterol, and remnant cholesterol — more precise breakdowns of the particle mix.
LDL particle number and size in some advanced panels.
Here is the key difference at a glance:

Apolipoprotein B (ApoB): Counting the Particles
Here is a concept that changes how you think about cholesterol. LDL-C tells you how much cholesterol is being carried, but it does not tell you how many particles are carrying it. Every atherogenic (plaque-forming) particle — LDL, VLDL, and remnants — carries exactly one molecule of apolipoprotein B on its surface. So measuring ApoB effectively counts the total number of harmful particles in your blood.
Why does this matter?
Because it is the number of particles battering your artery walls that drives plaque formation, not just the cholesterol they contain. Some people — especially those with diabetes, insulin resistance, high triglycerides, or the "cholesteroldepleted" small dense LDL pattern common in South Asians — carry a large number of small particles. Their LDL-C can look reassuringly normal while their ApoB, and therefore their real risk, is high. This mismatch, called discordance, hides risk that a standard report would miss entirely. The LAI treats LDL-C as the primary treatment target, non-HDL cholesterol as the co-primary target, and ApoB as a secondary target. ApoB is considered particularly valuable in people with diabetes, high triglycerides, obesity, or very low LDL who have already hit their LDL goal but may still carry residual risk. General ApoB goals used in aggressive lipid management are broadly:
Below 65 mg/dL for very-high and extreme-risk individuals
Below 80 mg/dL for high-risk individuals
Below 90 mg/dL for those at lower risk
If your LDL looks fine but your ApoB is elevated, that is a signal your doctor may want to intensify treatment.
Lipoprotein(a), or Lp(a): The Risk You Inherit
Lp(a) is one of the most underappreciated cardiovascular risk factors, and it behaves differently from everything else on your report. It is an LDL-like particle with an extra protein attached, and its level is almost entirely determined by your genes. Diet, exercise, and most standard cholesterol medications have little effect on it. You are essentially born with your Lp(a) level, and it stays fairly stable for life. High Lp(a) independently raises the risk of heart attack, stroke, and narrowing of the aortic heart valve — even in people whose LDL and everything else looks perfect. It is thought to be both pro-atherogenic (plaque-forming) and pro-thrombotic (clotpromoting). Because it is inherited, a high result also carries implications for your close family members, who may want to be tested
Two practical points follow from its genetic nature:
You usually only need to test it once in your lifetime. Since the level doesn't change much, the LAI notes that a one-time measurement is sufficient to assess this risk. There is currently no widely available drug specifically approved to lower Lp(a), though several are in clinical trials.
An elevated level means you should be more aggressive about everything else you can control — LDL, blood pressure, blood sugar, smoking, and weight. A commonly used threshold for concern is Lp(a) of 50 mg/dL (roughly 125 nmol/L) or higher, which is associated with a meaningfully increased risk of cardiovascular disease. Given how common elevated Lp(a) is in South Asians, testing it at least once is a sensible idea, particularly if heart disease runs in your family.
Apolipoprotein A1 and the ApoB/ApoA1 Ratio: The Balance That Predicts Risk
If ApoB counts the harmful particles, apolipoprotein A1 (ApoA1) counts the protective ones. ApoA1 is the main structural protein of HDL, the "good" cholesterol, and it does the useful work — pulling excess cholesterol out of artery walls and carrying it back to the liver, and helping keep the artery lining healthy. A higher ApoA1 generally reflects more functional protection, while a low ApoA1 signals that your defence system is weak. The real power comes from putting the two together. The ApoB/ApoA1 ratio captures, in a single number, the tug-of-war between the particles driving plaque into your arteries (ApoB) and the particles clearing it out (ApoA1). A high ratio means the harmful side is winning; a low ratio means your protection has the upper hand. Because it directly compares atherogenic and protective particles, this ratio often reflects true cardiovascular risk better than any single cholesterol value. Why this ratio deserves special attention:
It was the single strongest predictor in the INTERHEART study — a landmark investigation of heart attacks across 52 countries, including India and other South Asian populations. Of nine major risk factors examined, the ApoB/ApoA1 ratio carried the greatest predictive power for heart attack, outperforming every conventional cholesterol measure and every other lipid ratio such as LDL-C/HDL-C or total-cholesterol/HDL-C.
It works even when LDL looks normal. The ratio predicts the thickening of artery walls and the presence of vulnerable, rupture-prone plaque across all levels of LDL cholesterol, which is exactly why it catches hidden risk.
It is independent of age, sex, and ethnicity, and can be measured on a simple non-fasting blood sample.
It is directly relevant to us, since the INTERHEART data included South Asians, among whom this ratio is a robust marker of the premature heart disease we are prone to. Commonly used reference bands for the ApoB/ApoA1 ratio (laboratories may vary slightly) are roughly:

In short, a low ApoB paired with a high ApoA1 — a low ratio — is the profile you want. If your ratio is high, it is a strong signal to act on your modifiable risk factors and discuss treatment with your doctor, even if individual numbers on the basic panel look acceptable.

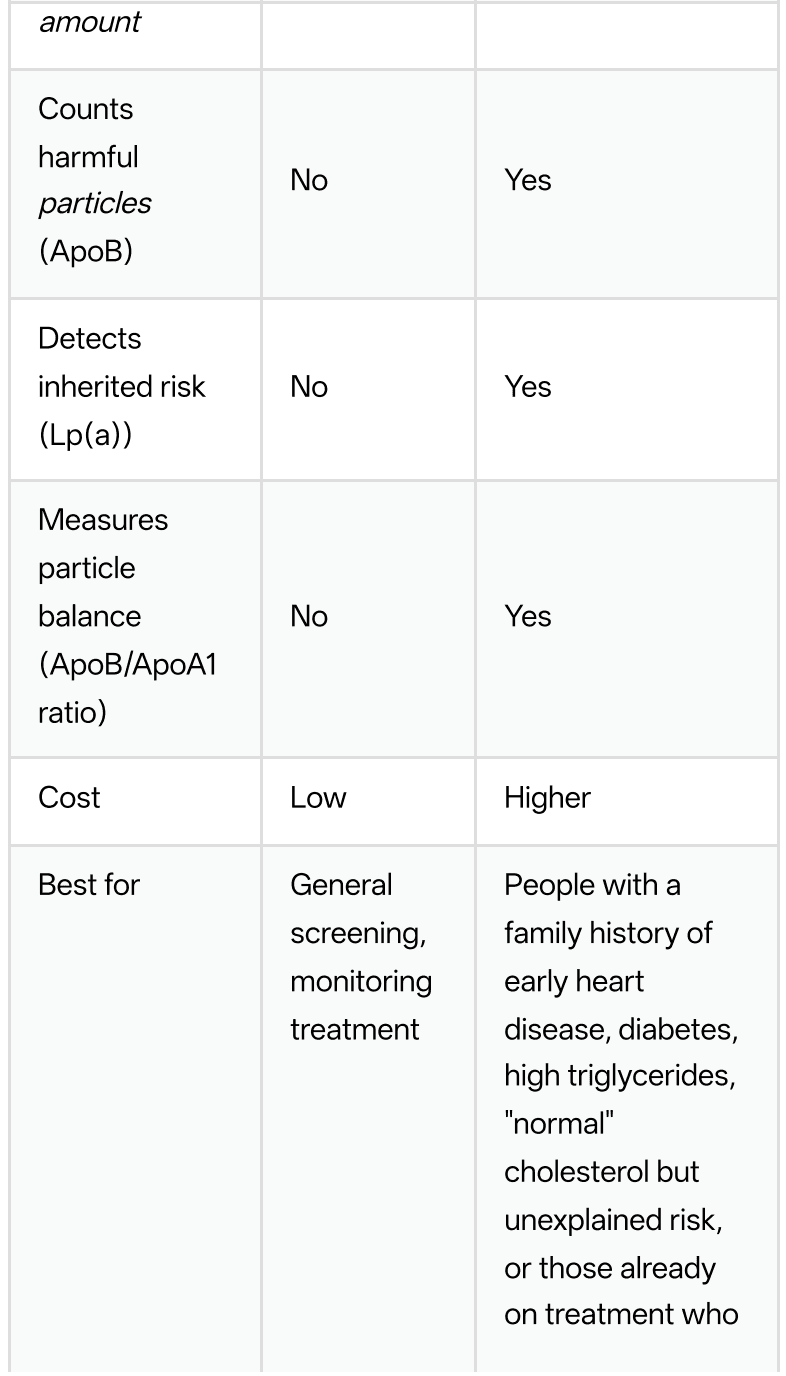
Putting It Together: LAI Risk Categories and Targets
The LAI does not use a single "normal" cholesterol level for everyoneInstead, your target depends on your overall risk. The higher your risk, the lower your LDL and non-HDL cholesterol need to go. This is why your neighbour's "acceptable" LDL might be dangerously high for you.What can make HbA1c read falsely LOW?
Extreme-risk categories apply to people such as those with established heart disease combined with familial hypercholesterolemia, diabetes with damage to organs, or those who keep having cardiac events despite already having very low cholesterol. These aggressive Indian targets exist precisely because our population develops disease earlier and more severely. As a simple guide, the non-HDL target is usually set about 30 mg/dL above the LDL target.
Physical Signs of High Lipids
Sometimes the body offers visible clues that lipids are running high, long before a report is ever ordered. Xanthelasmas are soft, yellowish, slightly raised patches that appear on or around the eyelids, especially near the inner corners — one of the most recognizable signs. Xanthomas are similar fatty deposits that can form over tendons (such as the Achilles or the knuckles), elbows, or knees. A grey or white ring around the coloured part of the eye, called corneal arcus, can also indicate high cholesterol when it appears in someone younger than about 45. These signs are not always present, and their absence certainly does not mean your lipids are fine — but when they do appear, they are worth taking seriously and getting your levels checked.
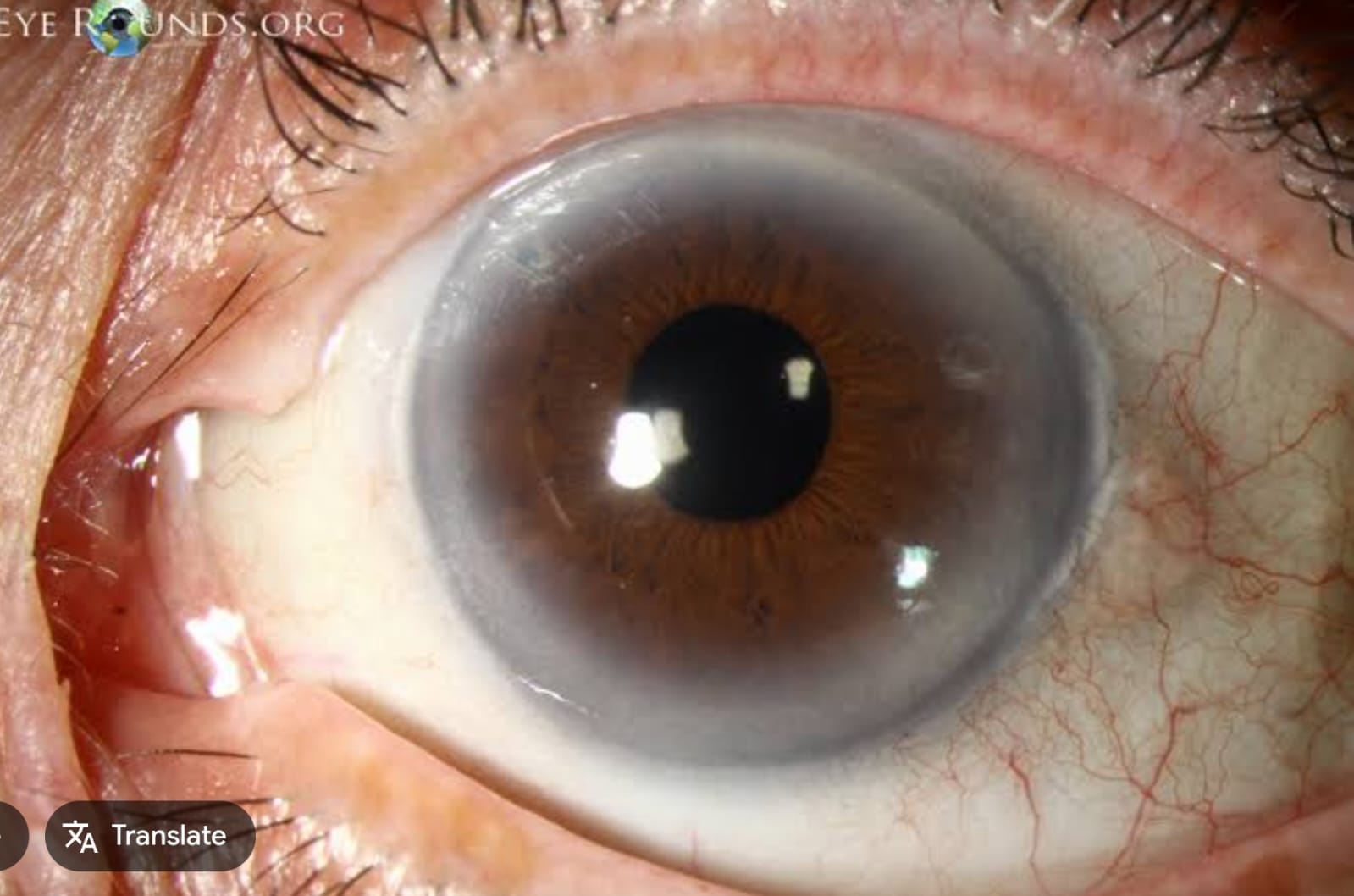
Corneal arcus: a grey or white ring around the edge of the iris, significant when seen before about age 45.

Xanthelasma — soft yellowish cholesterol deposits on the upper eyelid near the inner corner
Questions and Answers
Q: Do I need to fast before my cholesterol test?
Not usually. The LAI now considers a non-fasting sample adequate for managing most patients, which makes testing much easier. Your doctor may still ask you to fast if your triglycerides are very high or for a specific clinical reason. When in doubt, follow your lab's or doctor's instruction.
Q: My total cholesterol is normal. Does that mean my heart is safe?
Not necessarily. Total cholesterol is a crude average that can hide a bad LDL-to-HDL balance, high triglycerides, or a high particle count. It is entirely possible to have a "normal" total cholesterol and still be at meaningful risk. Look at LDL, non-HDL, and — if available — ApoB and Lp(a) rather than the total alone.
Q: What's the real difference between a basic and an extended lipid profile?
The basic profile measures the amount of cholesterol in different fractions. The extended profile adds markers that measure the number of harmful particles (ApoB), the protective particles (ApoA1) and the balance between them (the ApoB/ApoA1 ratio), and your inherited risk (Lp(a)). The basic panel screens and monitors; the extended panel explains hidden or unexplained risk.
Q: My LDL is at target, but my ApoB is high.What does that mean?
It means you likely have a large number of small, cholesterol-poor particles — a pattern common in diabetes, high triglycerides, and among South Asians. Each particle can still damage your arteries. A high ApoB despite a good LDL is a genuine red flag that your risk is higher than your LDL suggests, and it often prompts more intensive treatment.
Q: Should everyone get ApoB and Lp(a) tested?
Not everyone needs them at every visit, but they are especially worthwhile if you have a family history of early heart disease, diabetes, high triglycerides, or unexplained cardiovascular events. Because Lp(a) is genetic and stable, testing it just once in your lifetime is generally enough.
Q: Is a high HDL always good?
HDL is protective in general, but very high HDL does not give unlimited protection, and you cannot rely on a high HDL to cancel out a high LDL or ApoB. Focus on lowering the harmful particles rather than chasing a higher HDL number.
Q: How often should I get tested?
For healthy adults, screening every few years is reasonable, starting in early adulthood given the Indian risk profile. If you are on treatment, have diabetes, or have known heart disease, your doctor will test more often to confirm you are hitting your targets.
Q: Are the physical signs like xanthelasma reliable?
They are helpful clues when present but unreliable when absent. Many people with dangerously high cholesterol have no visible signs at all. Never use the mirror as a substitute for a blood test.
Q: My cholesterol looks fine, but my ApoB/ApoA1 ratio is high. Should I worry?
Yes, it is worth taking seriously. A high ratio means the harmful particles outnumber the protective ones, and this ratio was the strongest predictor of heart attack in the large, multi-country INTERHEART study — even better than standard cholesterol values. A high ratio despite an otherwise reassuring report is a genuine signal to tighten up your modifiable risk factors and discuss it with your doctor.
Key Takeaways
LDL-C is the main number to lower, but nonHDL cholesterol, ApoB, ApoA1, the ApoB/ApoA1 ratio, and Lp(a) together give a far more complete picture of your risk.
ApoB counts particles, which can reveal risk that a normal LDL hides — especially in diabetes, high triglycerides, and South Asians.
The ApoB/ApoA1 ratio weighs harmful against protective particles and was the strongest heartattack predictor in the global INTERHEART study; a low ratio is what you want.
Lp(a) is inherited, needs testing only once, and if high, means you should control everything else more aggressively.
Indian targets are stricter than Western ones because our risk starts earlier and runs higher.
Physical signs like xanthelasma can hint at high lipids, but only a blood test confirms it.
Your cholesterol report is a snapshot of your cardiovascular future — and one of the few health risks you can genuinely change. Read it, understand it, and use it as a starting point for a conversation with your doctor.
This guide is for general education and awareness only. It is not a substitute for professional medical advice, diagnosis, or treatment. Cholesterol targets, testing choices, and treatment decisions must be individualized. Always consult a qualified physician to interpret your own report and decide what is right for you
Up Next -