Diabetes
Understanding Your HbA1c Test Results
Written by - Dr. Nimisha Gupta, M.D. Pathology
10 min read
Learn what your HbA1c result means, how to interpret the numbers, what is considered normal, and the steps you can take to manage your long-term blood sugar health.

Before you start: This guide is for general education. It explains how HbA1c works and how to interpret a report, but it is not a substitute for advice from your own doctor, who knows your full history. Treatment targets and next steps should always be set with a qualified clinician. HbA1c is a sensitive result for many people. If reading yours brings up worry, that is a good reason to talk it through with your care team rather than sit with it alone.
What is HbA1c, in one sentence?
HbA1c is a blood test that estimates your average blood glucose over roughly the past two to three months — expressed as a single percentage.
What is actually being measured?
Glucose in your blood sticks to haemoglobin, the protein inside red blood cells that carries oxygen. Once glucose attaches, it stays attached for the life of that red cell. HbA1c measures what fraction of your haemoglobin has glucose stuck to it. The more glucose circulating in your blood over time, the higher that fraction climbs. Because red blood cells live for about 120 days (roughly four months), the test reflects a rolling average rather than a single moment. It is weighted toward the most recent weeks — the last 30 days contribute more to the result than the month before that — but in practice it is a fair summary of your last two to three months.
Why is this different from a normal blood sugar test?
A fasting or random glucose test is a snapshot — your blood sugar at one instant. It swings with what you ate, how you slept, whether you were stressed, and even the time of day. HbA1c is a summary. You cannot game it by fasting the morning of the test, and it does not spike because you were anxious in the waiting room. That stability is exactly why doctors rely on it to diagnose diabetes and to track control over time. One number, no fasting required, harder to distort.
Reading the numbers - What are the standard reference ranges?
Using the American Diabetes Association (ADA) thresholds, which most Indian and international labs follow:
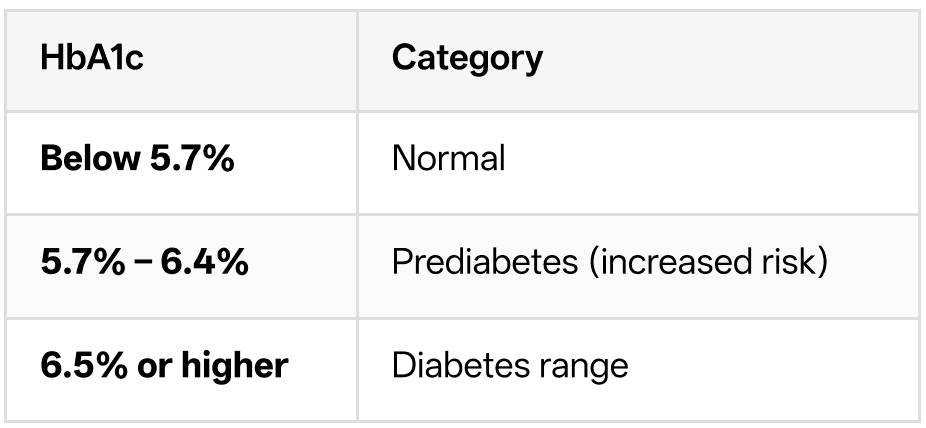
These cut-offs apply to a result from a properly certified lab. A single result at or above 6.5% usually needs to be confirmed with a repeat test on a separate day, unless you also have clear symptoms of high blood sugar. Your doctor makes the actual diagnosis — the number alone does not. A note on international variation: the ADA endorses HbA1c for diagnosing prediabetes at 5.7–6.4%. The World Health Organization is more conservative and does not endorse HbA1c for prediabetes diagnosis at all, while some European and Canadian bodies use a narrower 6.0–6.4% band. If your report cites a slightly different range, this is why. For most practical purposes in India, the ADA-aligned ranges above are the working standard.
My report shows a number in mmol/mol, not a percentage. What is that?
Some labs report HbA1c in mmol/mol (the IFCC unit) instead of, or alongside, the percentage. They measure the same thing on different scales. Rough equivalents:

If your report shows only mmol/mol, you can still use the same categories: 39 is the prediabetes threshold, 48 is the diabetes threshold.
What is the "estimated average glucose" (eAG) on my report?
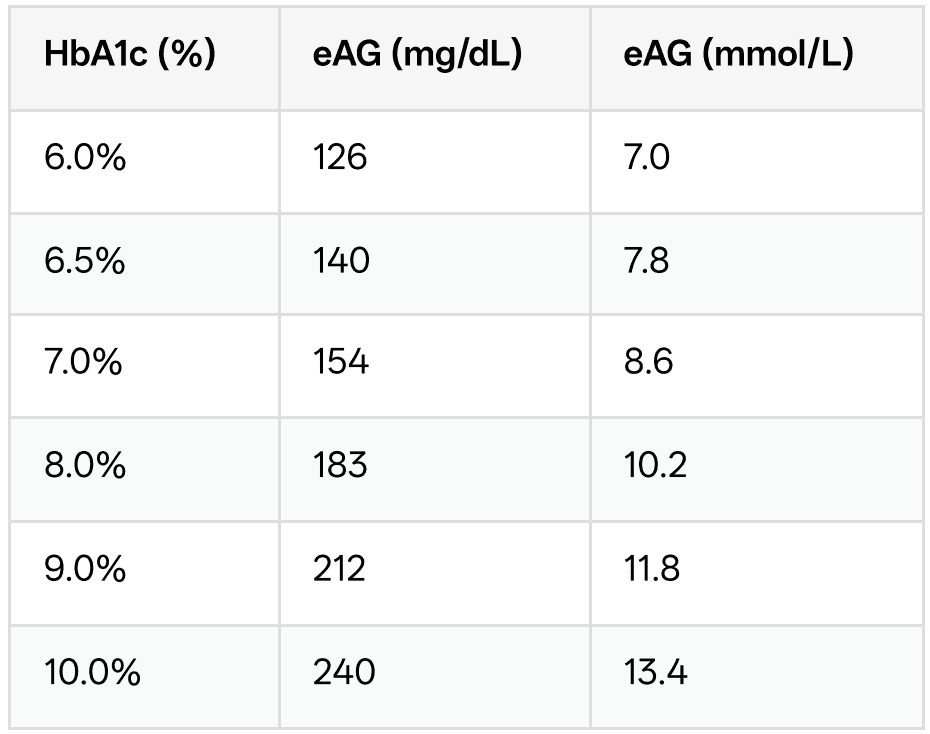
Many labs now print an eAG next to your HbA1c. This translates the percentage into the same units your glucometer uses (mg/dL), so it feels more familiar. It answers: "If my HbA1c is X, what has my average glucose roughly been?" The conversion comes from a large international study (the ADAG study) and uses this formula:
eAG (mg/dL) = 28.7 × HbA1c − 46.7
So an HbA1c of 7.0% works out to an eAG of about 154 mg/dL. Some useful reference points:
Why doesn't my eAG match the average on my glucometer?
This trips up almost everyone, so it is worth being clear: your eAG is unlikely to exactly match the average your meter shows, and that is normal — not an error. Two reasons. First, your meter only captures the moments you happen to test — often before meals, rarely at 3 a.m. — so its "average" is a biased sample of your day. The eAG is derived from continuous, round-the-clock data. Second, eAG is a statistical estimate. It gives a single point value but does not capture the variability underneath — the post-meal spikes, the overnight lows. Two people with an identical HbA1c can have very different day-to-day patterns. Treat eAG as a helpful ballpark, not a precise ledger.
What your result means for you ? My HbA1c is in the prediabetes range (5.7– 6.4%). Should I panic?
No — but do treat it as a genuine early-warning signal, because it is one. Prediabetes means your glucose is higher than normal but not yet in the diabetes range. It is the single most useful window you get, because it is often reversible. The evidence here is striking. In large pooled studies, people with HbA1c in the upper prediabetes band (around 6.0–6.5%) had a 25–50% chance of developing diabetes within five years. But that risk is not fixed. Structured lifestyle change — modest weight loss, regular physical activity, and dietary adjustment — has repeatedly been shown to sharply cut the chance of progressing to diabetes. Prediabetes is a fork in the road, not a verdict.
My HbA1c is 6.5% or higher. Does that definitely mean I have diabetes?
It means you are in the diabetes range and need to see a doctor promptly — but a formal diagnosis usually requires confirmation. Diabetes can be diagnosed by any of several tests: an HbA1c of 6.5% or higher, a fasting glucose of 126 mg/dL or higher, a 2-hour value of 200 mg/dL or higher on a glucose tolerance test, or a random glucose of 200 mg/dL or higher if you have clear symptoms. Except in cases with obvious symptoms, guidelines call for confirming the result with a second test on a different day, because no single test is infallible. Your doctor will also work out which type of diabetes and how to manage it. So: a 6.5%+ result is a clear prompt to act, not a moment to self-diagnose and self-treat.
What HbA1c target should I aim for once I have diabetes?
There is no universal target — and the ADA's recent guidance is explicit that this should be individualised, not one-size-fits-all. As a general orientation:
Below 7% is a common target for many nonpregnant adults.
Below 6.5% may be appropriate for some people, particularly if it can be reached safely without frequent low blood sugar.
Below 7% to 7.5% — a looser target — is often more sensible for older adults in good health, where the risk of hypoglycaemia can outweigh the benefit of tighter control.
The right number for you depends on your age, how long you have had diabetes, other health conditions, your risk of dangerous lows, and your own preferences. This is a conversation to have with your doctor, not a target to set from a chart.
How often should I get tested?
If you do not have diabetes and have no risk factors, screening every three years from around age 35 is a common recommendation, though many clinicians in India screen earlier given higher regional risk.
If you have prediabetes, roughly once a year to watch the trend.
If you have diabetes and are stable and at target, about twice a year.
If your treatment has just changed or your control is not yet where you want it, every three months, because that matches the biology — it takes about that long for a change in glucose to fully register in the HbA1c.
Testing more often than every three months rarely adds information, since the underlying red cells simply have not turned over enough to show a real shift.

When the number can mislead you - Can HbA1c ever be wrong or misleading?
Yes — and this is one of the most under-appreciated parts of the test. HbA1c depends on red blood cells behaving normally and living a normal lifespan. Anything that disturbs your red cells can throw the result off, sometimes substantially, even when your actual glucose control is fine. In these situations, doctors lean on direct glucose testing or a continuous glucose monitor instead.
What can make HbA1c read falsely LOW?
Broadly, anything that shortens red cell lifespan or increases red cell turnover — the cells do not survive long enough to accumulate glucose: Haemolytic anaemia (red cells breaking down early) Recent significant blood loss or recent blood transfusion Pregnancy, especially later stages Treatment that rapidly boosts red cell production (for example, iron therapy for iron-deficiency anaemia, or erythropoietin) Advanced liver disease
What can make HbA1c read falsely HIGH?
Broadly, anything that lengthens red cell lifespan or reduces turnover — cells hang around longer and collect more glucose:
Iron-deficiency anaemia (before treatment)
Vitamin B12 or folate deficiency
Advanced kidney disease (chronic kidney disease)
Recently having had your spleen removed
What about haemoglobin variants like thalassaemia or sickle cell?
This matters in India. Inherited haemoglobin variants — including thalassaemia traits and sickle cell — are relatively common in parts of the country, and they can interfere with certain HbA1c measurement methods, producing readings that are unreliable in either direction. If you have a known haemoglobin disorder, tell your doctor and the lab. Modern labs can often use a measurement method that is not affected by your particular variant, or your doctor may rely on fasting glucose, an OGTT, or a continuous glucose monitor instead. The key point: if your HbA1c and your dayto-day glucose readings tell very different stories, the variant may be the reason — investigate, do not just trust the percentage.
Taking action - Can I actually lower my HbA1c — and how fast?
Yes. The main levers are the familiar ones, and they work: consistent physical activity, dietary changes that reduce glucose spikes, weight management where relevant, good sleep, and — where prescribed — taking medication as directed. On speed: because HbA1c reflects two to three months of glucose, you will not see the full effect of a change for about three months. If you overhaul your habits in January, the March test shows the real result, not the February one. This lag is often discouraging to people who expect instant movement — but it is simply the biology of red cells. Be patient and consistent, and re-test at the right interval rather than chasing the number weekly.
What is a realistic first goal if my number is high?
For many people, aiming to bring HbA1c down in steady steps is more sustainable and safer than trying to crash it. Even a modest reduction meaningfully lowers long-term complication risk. And for those in the prediabetes range, the goal is often to get back below 5.7% and stay there — which lifestyle change alone can frequently achieve. Set the specific target with your doctor.
When should I see a doctor rather than just track the number myself?
Book an appointment if:
Your HbA1c is 6.5% or higher, or newly in the prediabetes range. Your number is rising over successive tests, even within a "normal" band.
Your HbA1c and your home glucose readings strongly disagree — this can signal a red cell or haemoglobin issue worth investigating.
You have symptoms of high blood sugar: unusual thirst, frequent urination, unexplained weight loss, fatigue, or blurred vision.
You already have diabetes and are consistently above your agreed target.
The five things to remember
1. HbA1c is your two-to-three-month average, not today's snapshot — which is exactly why it is trusted for diagnosis and tracking.
2. The bands are simple: below 5.7% normal, 5.7– 6.4% prediabetes, 6.5% and above the diabetes range — with a confirmatory test usually needed.
3. eAG is a friendly translation into glucometer units, but it will not exactly match your meter, and that is fine.
4. The number can mislead if your red cells are abnormal — anaemia, pregnancy, kidney disease, and haemoglobin variants (relevant in India) can all distort it. When HbA1c and daily readings disagree, dig deeper.
5. Changes take about three months to show up. Be consistent, re-test at the right interval, and set your personal target with your doctor rather than from a table.
This guide reflects widely used ADA-aligned diagnostic thresholds and the ADAG-derived eAG conversion. Ranges, targets, and interpretation should always be confirmed with your own clinician, who can account for your individual history